COVID-19 has changed the world as we know it. However, the pandemic has significantly affected the lives of people with disabilities, with many facing additional barriers in access to services, increased isolation and increased risks of poor health and social outcomes. To strengthen pandemic responses for all, it is crucial to understand the impact of COVID-19 on people with disability from their own perspective.
To help to address this gap, Shahreen Chowdhury worked with people with disabilities and caregivers in Bangladesh and Liberia as co-researchers, on ‘Pandemic Portraits’ – a project that aimed to prioritise their views by documenting their own lived experiences of COVID-19.
Using photovoice as a creative participatory methodology, co-researchers took photographs to capture their lived experiences through their lens. The collections of photos cover themes relating to inaccessibility, social connection, barriers to healthcare as well as nature, community, and spaces of healing.
“This is a picture of my sister playing basketball in the afternoon. We are homebound in this COVID-19 period. So, I try to spend good time with my family. If there was no lockdown, we would have been busy and I could not spend quality time with my sister. I am happy to see the smile on her face.” Israt Jahan Isha, 18-year-old, female caregiver of sister with physical disability, Bangladesh
“Due to the lockdown, I was not able to take my son for treatment as early as possible. The road is blocked… there are strict restrictions on public movement. Since last year, we are facing this challenge. I cannot take him anywhere for treatment…” Bithi Akter, 30 year old female caregiver of son with cerebral palsy, Bangladesh
“In this pandemic, I and my family members have tried to eat various types of fruits because we all know that it helps to strengthen our immune system. That’s why, we are trying to eat native fruits with vitamin C. And I want to say everyone to eat more fruits and plant more trees in this pandemic.” Saddam Hossian, 25-year-old male, Manikganj, Bangladesh
Photovoice, through imagery and storytelling, is a powerful tool in prioritising the voices of disabled people, adding to an evidence base to inform inclusive pandemic responses.
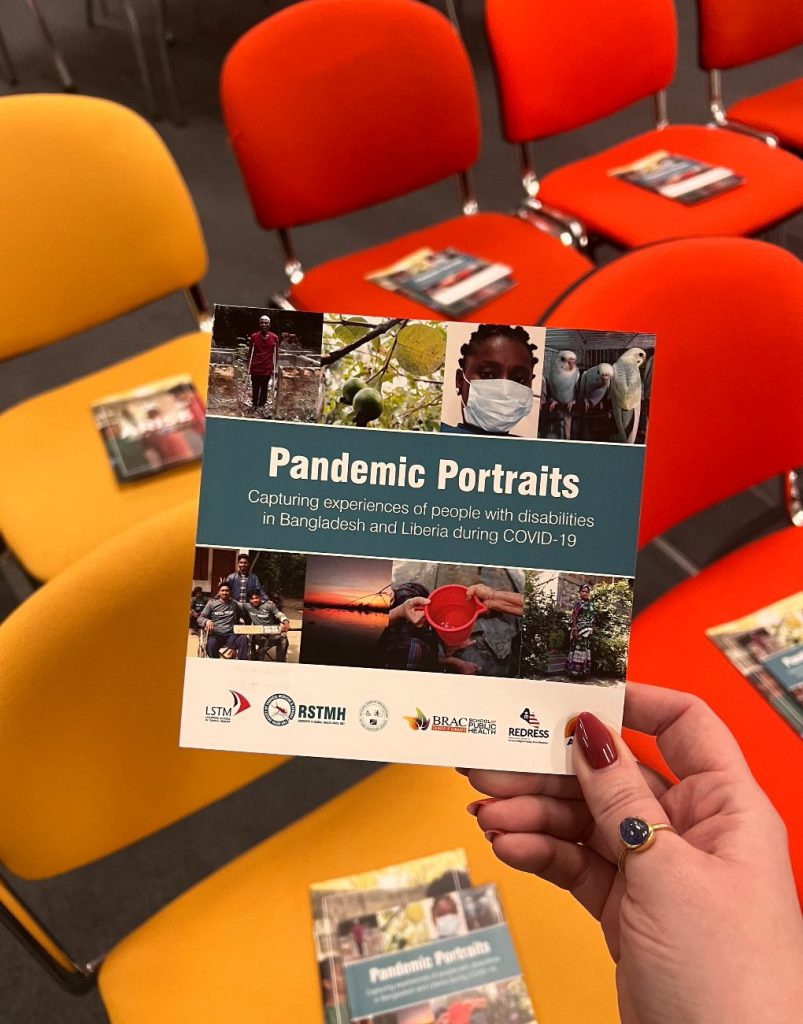
The Pandemic Portraits exhibition
The Pandemic Portraits project is linked to the ARISE (Accountability and Responsiveness in Informal Urban Settlements for Equity) project, of which IDS is a partner. On 23 January, 2023, IDS hosted a launch event for a ‘Pandemic Portraits’ a photovoice exhibition, which will be on display in the IDS Staff Common Room from January – March 2023.
The launch event brought together a range of stakeholders, including researchers and students from across IDS and Liverpool School of Tropical Medicine, providing opportunities to make connections and find synergies across the diversity of research that participants undertake on the issues of inclusion and disability.
In 2021, I took part in a diabetes storytelling workshop that supported awareness building efforts to prevent diabetes in India. About fifty participants – a diverse group of writers, researchers, and media artists – gathered to develop proposals for creative solutions for diabetes prevention. These proposals would then be presented to a panel of judges who would choose the most practical idea and award the team a grant to implement it in real life.
Over a couple of weeks, we had morning sessions where doctors, social activists, journalists, and people living with diabetes shared their views on the most urgent requirements to address diabetes.
In the evenings, my team from Lucknow, Guwahati and Chennai would ideate on a digital board, rehashing important points and what could be achieved within the duration of the project.
We filled our board with numbers and figures. There were arrows, circled words, text boxes, problem statements, references to reports and studies, and more. We decided to focus on the growing burden of diabetes among the urban poor.
We thought we had zeroed in on a problem to fix. We figured most people from the slum were working as domestic workers, battery-operated rickshaw drivers, or were involved in jobs that required sitting or minimal walking throughout the day. Their daily routines were such that they often ended up consuming sugar-laden things like chai, packaged biscuits, or chips, instead of home-cooked food.
Our subject expert, a doctor working with primary health centres in the villages around Lucknow, confirmed that we were on the right track. So, confidently, we decided to centre our awareness-building solution around WhatsApp messages or a wall painting campaign involving community members. .
Our confidence in our problem-solving skills was quite short-lived. It was only when we actually visited an urban slum that we realised that we were way off the mark.
Visiting urban informal settlements
We visited an urban slum that was next to a disused railway track with overgrown shrubs. The area was dotted with blue-yellow tents crafted from tarpaulin sheets. And we found people sitting in small groups puffing bidis.
We thought we would speak to the people and figure out which of our possible solutions would work best for them. We asked a group of young people how they go about their day – what they do/did for a living, what they eat, how and where they go for doctor consultations when they fall sick.
An old man from the bidi group closest to us overheard the discussion and promptly added, “Sabse achhi dawa wahan milti hai.” (The best medicine is available over there) and pointed towards the other side of the track.
A girl standing next to me explained he meant liquor, not actual medicine.
The old man added, “itne baras hogaye hum kabhi kisi dactar ke paas nahi gaye. Kuchh nahi hota hai dawa se” (It has been many years since we visited a doctor. Medicines don’t help.).
I can’t recall if we asked him any question after that. After all, our target population was the 18-35 year olds. I was more interested in learning what they thought about health, nutrition, and food habits.
As the answers started pouring in, I started striking out possible campaign ideas in my head until we were left with nothing.
They told us that they don’t have permanent jobs. Most of them go to the labour market and offer services in exchange for money. The pandemic had already worsened their limited work opportunities. Since they were not skilled, they were paid a very nominal wage for a day’s work; a pittance really. The women usually worked as waste pickers – collecting mostly plastic from different dumping grounds.
All of this indicated that they clearly did not lead sedentary lives. I made a mental note: “Strike out promoting more physical activity.”
The group said that their day often starts as early as 4am. Any two family members would cook for everyone in the household. They avoided sugar in their tea. On days when they had money, they would consume fish. But there were days when they stayed hungry for the entire day. They sometimes bought small biscuit packets while at work, but that was very rare. Another mental note to self: “Strike out any suggestion on nutrition.”
Except for one person who had an analogue phone, none of the others had a cell phone. There was just one person in their community who had a smartphone. Another mental note to self: “Strike out picture/ video messages on WhatsApp.”
Their homes did not have any walls. So, next mental note: “Strike out wall paintings.”
There were no proper shops in this area, except for one shop that sold bidi and pan. There were no vegetable or fruit sellers around.
People living in this area had no access to regular water supply or toilets. There was a common tap that was operational only at certain hours everyday, and people had to queue up to collect water for bathing and cleaning.
One of the women from the group thought we could help with their Aadhaar card (a biometric unique identification document in India) problems. She had lost hers because of flooding in her village. Now, she had no proof of identity to access her monthly ration entitlements.
We then went to another group of settlements, just two lanes away, and this place matched our target group.
Homes were made of more permanent materials (like concrete or brick), and people were able to avail their ration entitlements.
Most of the women were homemakers who spent a lot of time watching television. Children consumed packaged food like chips, biscuits, and pasta on almost a daily basis. Most of the men were e-rickshaw pullers or small stall owners, who spent most of their day sitting. These men often consumed street food instead of carrying home-cooked meals.
In fact, all of them had some idea about diabetes. A woman told us how her brother-in-law, an e-rickshaw driver, had been recently diagnosed with ‘sugar ki beemari’– a colloquial term for diabetes.
All children in this area attended schools nearby, and even used smart devices to continue their education online during COVID.
We were baffled by the stark contrast between these two settlements barely 500m apart. We realised that our diabetes messaging was far from perfect.
Adapting our proposal
Over the next couple of days, we incorporated our learnings and came up with a new idea: an approach centred on nutrition.
We proposed a highly complicated plan to create a series of a-day-in-the-life videos for policymakers. We thought it was important to show a snapshot of the lived realities of people living in informal settlements. These videos aimed to highlight the nutrition issues in both settlements: access and affordability of different kinds of food, access to healthcare, problems related to active/sedentary lifestyles, existing solutions and their drawbacks/successes.
We also thought of using Twitter storms to amplify the messaging and link it with the Government’s ‘Eat Right India’ campaign.
Overambitious and complex, I agree. But, the comments from the panel did not talk about the complex nature of this proposal nor did they say that we were targeting the wrong kind of slums.
Instead, the judges felt that policymakers already know what is to be known and that our videos would not be useful for the community. Three out of the four judges told us that a movie (or short movies) for the target community delivered to their phones via WhatsApp or something on those lines would have been a better solution, and even empower the community.
All I could think was- they don’t have smartphones!
Our solution was far from perfect. But, it bothers me that even within the proposal we presented, the informal slum dwellers and their issues were invisible to the panel. Just like the yellow-blue tents that are present in every city, but conveniently ignored and hidden when dignitaries pay a visit once in a blue moon
Join us for the launch of ‘Pandemic Portraits’, a photovoice exhibition, hosted by ARISE, telling the stories of people with disabilities in Liberia and Bangladesh living through the COVID-19 pandemic. This project was funded by RSTMH and completed in collaboration with REDRESS, Liverpool School of Tropical Medicine; the James P Grant School of Public Health, Bangladesh; and the National Union of Disabled, Liberia.
Date and time: Monday, 23 January 2023, 5.30 – 7.30pm
Location: Institute of Development Studies, Convening Space, Brighton, BN1 9RE
Please ensure you RSVP, for catering and accessibility purposes
The exhibition tells a visual story of the experiences of people with disabilities through their own eyes and words. Shahreen Chowdhury, a PhD researcher within the Social Science, Chronic Disease and Disability Unit at the Liverpool School of Tropical Medicine worked with co-researchers in Bangladesh and Liberia. Using photovoice as a creative participatory methodology, co-researchers took photographs to capture their lived experiences through their lens. The findings present themes relating to inaccessibility, social connection, barriers to healthcare as well as nature, community, and spaces of healing. Photovoice, through imagery and storytelling, has been a powerful tool in prioritising the voices of disabled people, adding to an evidence base to inform inclusive pandemic responses.
Short presentations will be followed by snacks and drinks, and the opportunity to view the exhibition and speak with the presenters, including Shahreen Chowdhury who undertook this research in partnership with Salma Akter Urme, Boakai A. Nyehn Jr, Heylove R. Mark Sr, and co-researchers.
Speakers:
Hayley MacGregor – Professorial Fellow, Institute of Development Studies
Shahreen Chowdhury – Research Assistant and PhD student, Liverpool School of Tropical Medicine
Boakai A. Nyehn Jr, Heylove R. Mark Sr and Salma Akter Urme – Co-researchers from National Union of Organizations for the Disabled Liberia and BRAC James P Grant School of Public Health
Stephen Thompson – Research Fellow, Institute of Development Studies
ARISE Disability Working Group member (speaker TBC)
Covid-19 protocol
The wearing of masks is voluntary, and we encourage those who would like to wear masks to do so. Surgical masks are available in many of the meeting rooms and from the reception counter. If you are planning to attend an event and would like to request that others wear a mask, you can either contact us in advance at cet@ids.ac.uk, or speak to an IDS representative on the day.
We also ask that when requested by colleagues or others in a meeting or event to wear a mask, please treat the request with respect and put a mask on.
If you are feeling unwell or have any Covid-19 symptoms, please do not come into the IDS building.
As we move into the new year, we wanted to reflect on a very busy 2022 for ARISE. To recap on some of our work from this year we are counting down our top 10 most popular blog posts and pages on the ARISE website from the last year.
In this blog post Jacob Omondi explains issues leading to youth related crime and violence in the Mathare Valley area of Nairobi, and explores some solutions for helping youth find meaningful ways to stay away from crime and earn a living.
On World Menstrual Hygiene Day 2022, we reflected on the impact that menstruation, and the social stigma around menstruation, have on the lives of women waste workers in India.
This blog post details a workshop where stakeholders discussed the health, wellbeing, housing and water and sanitation related challenges faced by the residents and the governance systems in urban informal settlements. The blog post notes that while there are many problems, there is no comprehensive national urban policy which addresses these issues.
This blog discusses how the ARISE team at African Population and Health Research Center (APHRC) supported the inaugural Youth & Women in WASH conference in Naivasha, Kenya, where the theme was ‘Unlocking potentials of Youth and Women for Sustainable Water and Sanitation Services.’
For many slum dwellers, state relocation programmes are probably the only gateway to moving out of dangerous living conditions. But are they happier after moving out? Do their lives improve? Do their aspirations change? Do their perceptions about life change? In this blog post ARISE aims to answer some of these questions.
‘Urban informality’, Roy argues, is “a state of exception from the formal order of urbanization”. Thus, urban informality is often confined to the urban poor – informal settlements are not formally acknowledged or regulated by local or city authorities, and residents often lack title deeds.
This section of our website is focused on our work on Community-Based Participatory Research (CBPR). It’s a place where you can read updates on our work and also hear about some of the challenges we have faced.
In this blog post we discuss the fact that violence within slums is not inevitable. It is the consequence of structural violence against poor and marginalized people and state responses that exacerbate the problem.
In February, World Day of Social Justice gave us the opportunity to reflect on and highlight the need for social justice for marginalised communities like those involved in waste work in urban spaces. And so ARISE launched the Voice Quilt – a novel multi-media project that brings the voices of individual waste workers to the fore, reflects their various concerns and desires, and highlights the importance of achieving social justice for those working in the world of waste.
In this blog Rosie Steege, Jane Wairutu and Linet Okoth report back on the passing of the Nairobi City County Community Health Services Act in June 2021 – welcome news for Nairobi’s Community Health Volunteers (CHVs) who have waited almost two years since the Bill’s inception.